
Dr.K. Kalaivani
Director/HOD
List of Faculty
Institute of Obstetrics and Gynaecology was the first allopathic maternity hospital in British India to address women's reproductive health. There is perhaps no other acreage in Egmore that is as filled with hope as this hospital. The Institute of Obstetrics and Gynaecology (IOG) and Government Hospital for Women and Children, fondly called MH (maternity hospital) by generations of doctors, nurses, students and allied staff is a tertiary healthcare centre. Age (189-years old) has not defeated its ranks and it has gone above and beyond doing what it was first founded for in 1844 – delivering babies.
It was established on the banks of the Cooum near the Egmore Railway Station under the superintendentship of stalwarts such as Drs WS Thompson and James Shaw — who instituted a professorship in midwifery at the Madras Medical College — but moved to its present location on Pantheon Road in the 1880s because of the annual flooding of the river.
Laid out in the shape of a female pelvis, the new structure came up on Pantheon Road, under the guidance of Major General G.G. Gifford, who is commemorated with a block in his name on the campus. The new hospital was completed in 1881 in Egmore and by 1900 had expanded to five blocks with a total of 140 beds. IOG has conducted so many difficult deliveries. the imprisoned former-Queen of Burma – Supayalat – gave birth in IOG after a long and Excruciating labour. IOG hospital has delivered the exiled queen, Supayalat, of Burma in the late 1800s and also actors such as Vijay.
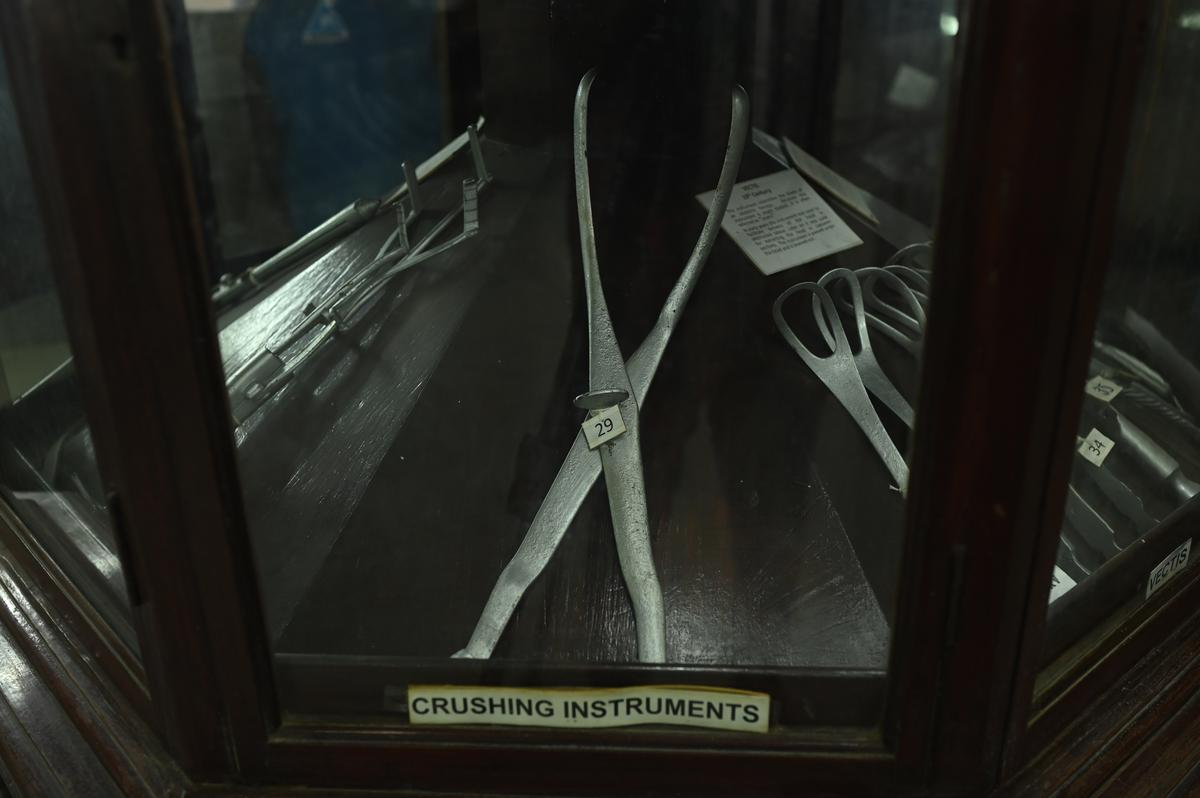
The Gifford School named after Major General Gifford, a former superintendent of the hospital still remains untouched which was setup in 1911. It has the most fascinating specimens and ancient obstetrics instruments.
The hospital was to be headed by several noted medical practitioners. IOG hosted the first All-India Obstetrics and Gynaecological Congress in 1936. The venue was the Museum Theatre and inaugurating it was Dr.Ida Scudder of CMC Vellore, with Dr. Sir A. Lakshmanaswami Mudaliar in the chair. He was also the first Indian to be the Superintendent of IOG, occupying the post between 1939 and 1942.
When it was constructed, the buildings resembled the shape of women's pelvis and sacrum. But over the years, portions were demolished to make way for multi-rise buildings that could accommodate more patients. Dr. AL Mudhaliar, was the first Indian to head the hospital in the years before the second world war. Earlier, the red brick wings had large high sealing rooms, broad verandahs that lead to a statue of a mother and child. Today, much of that has been replaced by waiting area and AL Mudhaliar block. Now IOG has 1075 beds with 95%-100% occupancy and now has separate building for Obstetrics and Gynaecology. AL Mudaliar block is for obstetrics
New building is opened from July 2022 exclusively for Gynaecology and Fertility OPD. VIA, VILI and Colposcopy facilities are available at gynaec OPD. Has separate Operation theatres for Gynaecologic surgeries including laproscopic and endoscopic surgeries in that new building. Pre-operative and Post-operative gynaecology wards is there in the same building.
Standing proudly, IOG Egmore has departments Surgical Oncology, Medical Oncology, Radiotherapy, family planning, assisted reproductive techniques, Endocrinology apart from conducting cities most high risk deliveries.
IOG, Egmore to get 1st Public Fertility treatment centre with IVF facilities. To the relief of thousands of poor patients who otherwise cannot afford infertility treatment in private hospitals, the State government on 28th April 2023 announced that it will establish infertility clinics that offer in vitro fertilisation (IVF) treatment at the Institute of Obstetrics and Gynaecology in Egmore at a cost of Rs 2.5 crores. 2nd floor of the Gynaec-Surgical block is completely dedicated to fertility clinic. As of Now Ovulation induction and IUI is being done at FRC OPD. SSG, HSG, DHL, septal resection and other necessary treatments available are being given to the patients.
The hospital became a teaching centre with postgraduate and diploma courses in 1930 under the Madras Medical College. In 1952, it became one of three postgraduate institutes of Madras city, and that marked the beginning of the Institute of Obstetrics and Gynaecology at the Maternity Hospital. Dr. R.K.K. Thampan was the first Director.
This Institute has intake of 55 post-graduates/year. This hospital is recognised as a centre of excellence, conducts around 15,000 – 20,000 deliveries annually. Most of them being high risk cases.





Dr.K. Kalaivani
Director/HOD
List of Faculty
| S.No | Name of the Residents joined in the year 2020 | Name of the Residents joined in the year 2021 | Name of the Residents joined in the year 2022 |
|---|---|---|---|
| 1 | - | - | - |
| 2 | Dr. Mohamed Ismail |



| S.NO | Date | CME / CONFERENCE – Title | University / TNMSC Credits / both if present | State or National level or institute level | Related Images |
|---|---|---|---|---|---|
| 1 | 24.2.2022 | CME on recent advances in gynaec oncology surgery | - | STATE LEVEL |



| S.NO | Date | WORKSHOP / TRAINING with Title | University / TNMSC Credits / both if present | State or National level or Institute | Related Images |
|---|---|---|---|---|---|
| 1 | 22.06.2022 | Workshop on ENDOGYNAECOLOGY | - | STATE LEVEL |
| S.NO | Date | Quiz / Competitions with Title | University / TNMSC Credits / both if present | Prizes awarded to |
a. Inter or Intra – Collegiate Level b. State or National level |
Related Images |
|---|---|---|---|---|---|---|
| 1 | 04.08.2023 | BREAST WEEK FEEDING QUIZ | - |
Dr. Sangeetha Dr. Sivasankari Dr. Kaviya |
INTRA COLLEGE |
| S.NO | Date | Other events with Title | Details | Related Images |
|---|---|---|---|---|
| 1 | - | - | - |
| S.NO | Date/Month & Year | Name of the Awards & achievements received | Name of the awardee with designation | District level / State level / National level | Images |
|---|---|---|---|---|---|
| 1 | 02/01/2020 | FIRST PRIZE IN POSTER ON TNFOGA | DR.RAMYA JUNIOR RESIDENT | District | View |

Topic: UROGYNAECOLOGY & PELVIC SURGERY
STATE LEVEL

Topic: MENOPAUSE MANAGEMENT
STATE LEVEL

Related Images1

Related Images2
UROGYNAECOLOGY & PELVIC SURGERY
Related Images1

Related Images2
MENOPAUSE MANAGEMENT
We are proud that IOG, Egmore is LaQshya certified centre. On May 2023 we received National LaQshya certification. Proud and happy to offer Public good respectful care and with good Infrastructure. All doctors and staffs are LaQshya trained.
29 year old Prmigravida, Mrs.X 20 weeks of gestation, was referred to tertiary centre for management of ovarian cyst complicating pregnancy. USG showed multi-loculated cyst with septations in left ovary. Lesion was found to be progressively increasing in size. MRI done which revealed T2 hyperintense lesion of size 6.75x6cms with multiple septations in the left ovary. Tumor markers were done and found to be raised. CA-125- 671.
Surgical oncologist and medical oncologist opinion was obtained and uterus sparing staging laparotomy was done in mid-trimester at 24weeks. Pathological results revealed Micro-papillary variant of serous carcinoma – invasive type with omental deposits. – STAGE III A. Post operatively patient was given 4 cycles of chemotherapy antenatally. (Carboplatin x 2 cycles and Carboplatin with cyclophosphamide x 2 cycles). Elective LSCS along with Right salpingo-ophrectomy was done at 38weeks. After LSCS patient received 2 cycles of Chemotherapy. Patient is now under regular follow up in medical oncology with no recurrence. Mother and baby are healthy.
A 33 years old primi Ms-1Year 147 cm/LMP 23.8.20 EDD 30.5.2021 presented in AN opd with single intra uterine gestation of 35w+6 days.
History of viral illness 6-7 years back followed by weakness of lower limbs with difficulty in walking/squatting position/combing hair/buttoning dress H/o of sibling who died of muscular dystrophy (respiratory depression) Patient had tested Covid positive Primary cesarean section done, Boy baby. Weight – 2.6 kg. Post partum, Mother and baby was healthy.
A Case of 28years old, G2P1L1, Previous one LSCS presented at 32 weeks with complaints of breathlessness for one month, aggrevates on walking for few steps, (NYHA – 111). Admitted in ICU, Echo done and was found to have severe Pulmonary Hypertension (TRPG-72mmHg). Rheumatology opinion obtained, found to have connective tissue disorder – Anti-SS-A and Anti-SS-B Positive. Patient was started on diuretics, Vasodilators(T.Sildenafil), HCQ, Steroids and MgSO4 for neuroprotection. Emergency LSCS done with Cardiologist standby under general anaesthesia at 32weeks + 4 days. Intra-op and Post-op period was uneventful. Post operatively cardiologist opinion obtained and T.Bosentan was started. Appropriate treatment with Multi-disciplinary approach at right time had saved mother’s life. Now she is in regular cardioilogy follow up. Alive and healthy. T.Bosentan 10 tablets costs 800 rupees. But this all medications was given free of cost in IOG and RGGGH.
Retroperitoneal tumours originating from retroperitoneum without originating from major organs are rare. 70-80% of the primary retro-peritoneal tumours are malignant. Most common malignant tumours in this region are sarcomas. Most common benign lesion is lipoma and fibromas.
No Centarl Lab information available for this department.
No Highlights information available for this department.
No High Dependency Unit information available for this department.
No Others information available for this department.
